You have probably seen the viral videos of humanoid robots doing backflips, pouring lattes, or mimicking human conversation. They look cool, but they always felt a bit like expensive party tricks.
That just changed.
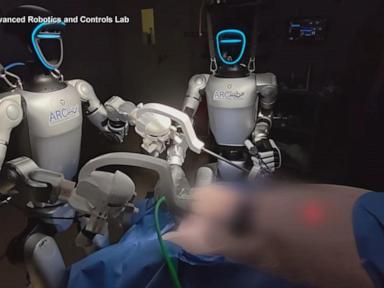
Researchers at the University of California San Diego just did something that actually matters. They took a commercial Unitree G1 humanoid robot, nicknamed it "Surgie," and used it to assist in removing a gallbladder. This was not a pre-programmed simulation. It was a live, preclinical trial on non-primate mammals, and it marks a fundamental shift in how we think about medical automation.
If you are wondering why anyone would force a two-legged, human-shaped robot into a crowded operating theater when we already have multi-million dollar surgical machines, you are not alone. But the truth is, the current medical system is hitting a wall.
What Most People Get Wrong About Robotic Surgery
When people think of robotic surgery, they think of the DaVinci system. It is an impressive piece of engineering, but it has a massive scale problem.
Current multi-armed surgical systems are beasts. They weigh upwards of 1,800 pounds. They require dedicated, retrofitted operating rooms, custom infrastructure, and specialized teams just to keep them running. They also cost millions of dollars. Because of this, these machines stay locked away in wealthy, urban medical centers.
If you are in a rural clinic, on a military battlefield, or in an under-resourced community, that technology might as well not exist.
Surgies, on the other hand, stand about five feet tall and weigh only 60 pounds. They do not need a custom room. They are built to occupy the exact same physical footprint as a human nurse or assistant.
+------------------------+------------------------+
| Specialized Systems | Humanoid Bots (Surgie) |
+------------------------+------------------------+
| Weight: ~1,800 lbs | Weight: ~60 lbs |
| Cost: Millions | Cost: Fraction of tech |
| Needs custom OR suite | Fits standard human space|
| Single-purpose design | Adaptable / Multi-task |
+------------------------+------------------------+
The AI Training Advantage
The real magic isn't just the physical size. It is the data.
Right now, training a traditional surgical robot to be autonomous is almost impossible. The scale of medical data required to teach a highly specialized machine is too labor-intensive and expensive.
Industrial humanoid robots, however, are seeing a massive explosion in AI foundation models. Tech companies are pouring billions into teaching bipedal robots how to grip, navigate, and interact with the world.
By using a humanoid form factor in the hospital, medical researchers can piggyback on all that industrial AI data. A robot that learns how to gently hold a fragile object in a factory can use those same basic neural networks to hold an ultrasound probe or an endoscopic camera for a surgeon.
How the UCSD Trial Actually Worked
Led by engineer Michael Yip alongside surgeons Charles Goldberg and Preetham Suresh, the UC San Diego School of Medicine team ran a bimanual teleoperation system.
Let's clear up one major misconception: the robot did not make its own decisions. This was not an autonomous AI slicing into a patient.
Instead, a human surgeon controlled the robot from afar using motion capture technology, tracking systems, and foot pedals. The setup allowed the operator to coordinate both robotic arms simultaneously. The surgeon could hold tissue back with one hand while using the other arm to cut, perfectly mirroring human movement.
The team completed two gallbladder removals. One procedure paired a humanoid robot with a human assistant. The second procedure used a pair of robots working together.
It Was Not Perfect
We need to be honest about the limitations. This was a proof-of-concept trial, and early-stage tech is messy.
The team ran into immediate bottlenecks:
- The robots required recalibration multiple times during the procedures, which dragged out the surgery times significantly.
- Latency between the surgeon's hand movements and the robot's physical response needs serious refinement.
But context matters here. Think back to the early days of laparoscopic surgery. The very first machine-assisted laparoscopic procedures could take six hours. Today, doctors knock them out in 30 minutes. The UCSD team expects a similar trajectory for humanoid systems.
Where We Go From Here
Humanoid robots are not replacing doctors tomorrow. Widespread clinical use in human hospitals is still years away, requiring massive regulatory hurdles and extensive safety trials.
But you don't need full autonomy for these robots to solve the burning crisis in healthcare: staffing shortages.
Before a robot ever touches a scalpel on a human patient, it will likely start as a high-end scrub nurse. It will handle the low-risk, physically draining tasks that burn out human staff. It can hold heavy retractor tools for hours without getting tired. It can pass sterile instruments to the lead surgeon, or clean up the operating room after a grueling case.
If you want to track where this technology goes next, stop looking at the flashy humanoid walking videos. Watch the space where medical researchers are quietly adapting these machines for low-risk clinical assistance. The future of surgery isn't a solitary AI doctor; it is a collaborative operating room where humans and adaptable machines work side-by-side.



